Exoskeletons
Warning: Undefined variable $includes in /home/determined2heal/determined2heal.org/wp-content/plugins/intel_link_list.php on line 30
Support
Determined2Heal

Medical Benefits of Exoskeleton-Use
It comes as no surprise that daily standing accompanied by ambulatory walking movement comes with medical benefits, especially for those living with paralysis. Exoskeletons are improving paralyzed persons quality of life and health one step at a time. Below is a thorough paper discussing these medical benefits.
Medical Benefits and Safety of the ReWalk Exoskeleton System
Key Points:
- The use of an exoskeleton has been shown to restore ambulatory function in people with lower extremity paralysis due to a spinal cord injury or lesion.
- By utilizing an exoskeleton, community-based ambulation is a viable reality for people with lower extremity paralysis due to a spinal cord injury or lesion.
- Based on the clinical benefits that are derived from using a computerized exoskeleton (decreased pressure ulcers, improved bowel and bladder functions, decreased pain, among other things), we anticipate cost-savings for third-party payers can be achieved if patients can maintain or regain ambulatory function.
- The use of exoskeleton technology has been shown to be safe.
Introduction
The loss of upright mobility has a profound effect on the health and quality of life for individuals with a spinal cord injury (SCI). Paraplegia following SCI results in a variety of long-term medical complications, including lower extremity bone loss, pain, pressure ulcers, chronic sleep disturbances, urinary tract infections and difficulties with bladder and bowel evacuation. The economic impact of SCI is also substantial. As of 2014, about 30% of all SCI individuals required one or more hospitalizations each year, with an average stay of 23 days (1). The average annual healthcare cost and cost of living for SCI paraplegics is $510,883 for the first year after injury and $67,677 for each subsequent year, not including lost wages and benefits (1). For an individual who is injured at age 25, the estimated lifetime costs exceed $2.2 million. Rehabilitative measures aimed at improving the health and independence of SCI individuals are critically needed to reduce the escalating medical expenses associated with SCI.
One of the most fundamental goals of rehabilitation medicine is to enable the patient to resume walking. Ambulation is regarded as necessary and beneficial in the treatment of individuals with mobility impairments due to stroke, age or injury. In this respect, gait speed has been suggested to serve as the “sixth vital sign”, potentially predicting future health status and accurately reflecting physical changes (2). This concept has been extended to individuals with SCI, where walking speed is being used to estimate functional ambulation during daily life after SCI for motor incomplete individuals and to distinguish between ambulation categories with a high degree of sensitivity (3-5). With the advent of new robotic technologies to assist motor complete paraplegics with standing and independent ambulation, walking can be more universally used to assess and maintain the health of individuals with SCI. Robotic-assisted walking can be incorporated into the rehabilitation regimen for paraplegics with SCI, helping to maintain overall health and the specific health-related issues that result from loss of upright weight-bearing mobility.
The ReWalk exoskeleton is an FDA-cleared assisted walking device for SCI paraplegics. The ReWalk is a wearable, computer-controlled device that enables paraplegics to stand and walk using crutches to assist with balance (Figure 1). ReWalk users can autonomously determine walking initiation, speed and direction through a combination of controller commands and shifts in weight. The medical benefits and safety of the ReWalk computer-controlled exoskeleton for SCI paraplegics will be discussed in this review. The data available from early participants in ReWalk clinical trials show the safety of the ReWalk in as well as promising improvements in the medical issues associated with SCI. These results suggest that restoration of upright mobility may help mitigate the physical and psychological decline routinely experienced by individuals with SCI.
Health Benefits Associated with Walking
Walking has been widely promoted by the American Heart Association and other health organizations as a beneficial form of exercise that reduces the risk of heart

Figure 1: The ReWalk exoskeleton is a wearable, powered assistive device that allows paraplegics to stand, sit and walk independently.
disease, stroke and diabetes (6). A regular walking program also prevents weight gain and bone loss due to osteoporosis (7). Walking is an easily accessible activity for individuals of all ages and abilities. Exercise intervals as short as 10 minutes have been shown to be effective in helping to maintain and improve health (6).
The benefits of walking are particularly important for mobility-impaired individuals who otherwise experience a predominantly sedentary lifestyle. In addition to overall health maintenance, walking can provide a way to improve flexibility, muscle strength and circulation for these individuals. Upright mobility may also reduce the incidence and severity of pressure ulcers, which are an especially serious concern for paraplegics with SCI who spend the majority of their day seated in a wheelchair or in bed. Regular use of mobility assistance devices allows paraplegics to relieve compressive skin pressure more completely than simple padding or repositioning can achieve. In a study of the benefits of standing upright for SCI individuals, 33% of participants reported a decrease in pressure ulcers when the assistive device was used more than once per day (8). Upright mobility may be even more effective in improving skin blood flow and helping maintain skin health.
Walking with the ReWalk Exoskeleton
The ReWalk exoskeleton is intended to be used by individuals with SCI at levels from C7 to L5. The extent of the injury can be either motor complete or incomplete as described by the ASIA A or B criteria. The user must have bilateral upper extremity function that allows them to use crutches to assist in chair rising and walking. ReWalk users are trained extensively until they gain proficiency at independent use of the device. In ReWalk clinical trials (9,10), training was conducted three times per week and individual training sessions lasted up to two hours each. Training is progressive, with the basic goals of becoming skilled at device donning and doffing procedures, sit-to-stand and stand-to-sit transitions, standing balance and weight shifting, and finally indoor walking on a flat surface. Participant pace of advancement is self-regulated, according individual capabilities and confidence level. Trainer assistance is gradually reduced as the user becomes more accomplished in the device. Once fundamental walking skills are acquired, training progresses to more advanced mobility skills such as increased walking speeds, walking outdoors, and negotiating sloped surfaces, curb cutouts, and motorized doors.
Independent walking with the ReWalk exoskeleton involves user selection of the device mode on the wrist communicator. When walking mode is chosen and confirmed, the user initiates walking by moving the crutches forward and creating a “tilt” that is sensed by the ReWalk. In response, the device moves the right leg forward. Once the crutches are advanced again, the left leg is moved forward in front of the right leg. These motions are repeated to create the ReWalk gait. The user is in complete control of gait speed by determining when the crutches are moved forward to take the next step. Similarly, sit-to-stand and stand-to-sit transitions are determined by user interaction with the ReWalk via the wrist communicator.
The ReWalk is Safe and Effective to Use in Community Settings
The initial participants in ReWalk clinical trials were able to safely use the ReWalk in various community settings (17, 26) beyond a rehabilitation facility. Participants were able to achieve primary standing skills within one week and primary walking skills within five weeks of training. These participants were also able to transfer into and out of the device and manage the chest, thigh and calf straps independently after they received assistance with placing their feet in the shoes.
Following several weeks of training, study participants were able to use the ReWalk in various community settings as well as to conduct secondary indoor walking skills. From being able to retrieve an item from an overhead shelf to walking outdoors on different surfaces, users of the ReWalk were able to safely navigate through real world settings with minimal assistance. Specifically, participants were able to navigate indoor on tile and carpet and outdoor on concrete, pavement, grass, uneven ground surfaces, slopes and curb cutouts (17, 26).

Figure 2
Figure 2, 3: The ReWalk exoskeleton being tested in various community settings (17).
In sum, training participants were able to tolerate longer sessions and walk greater distances during each session (26). A higher level of efficiency was achieved for the exoskeletal-assisted walking with increased skill in using the device. Indoor and outdoor-specific exoskeletal mobility was shown to be velocity-dependent.
ReWalk Walking Biomechanics
Loss of weight-bearing mobility following SCI has an adverse effect on the bones in the lower extremities. Bone is highly sensitive to its cyclic mechanical strain environment, with site-specific variations in response (11, 12). The balance between bone formation and resorption is altered when strain reduced, resulting in disuse osteoporosis. Studies of bone mineral density (BMD) changes in individuals with SCI show that rapid initial bone loss occurs primarily in the trabecular bone of the lower limbs (13, 14). Trabecular bone loss slows about three years post SCI, while slower cortical bone loss continues long-term. The ongoing cortical bone loss correlates with the increased lower limb fragility fracture rate reported for SCI individuals at longer times post injury (14).
While it is well established that weight-bearing exercise prevents bone loss and increases BMD in post-menopausal women, the potentially protective effects of exercise are not yet clear for SCI individuals. The magnitude of bone loading and the resultant cyclic bone strains from various passive weight bearing methods reported in the literature may be insufficient to restore the normal balance between bone resorption and bone formation. Similar insufficiencies may also exist in the supine exercise programs used in bed rest studies. These studies are further complicated by wide variations in time since SCI. Longer term SCI individuals with ongoing cortical bone loss may not respond in the same way as shorter-term SCI individuals with predominantly trabecular bone loss. Eliminating the complicating factors associated with SCI, disuse studies and studies of astronauts exposed to microgravity conditions demonstrate that recovery of bone mass is possible with reambulation after short-term disuse (15, 16). Bone recovery begins quickly, but may take years to complete or remain incomplete. The amount of bone mass recovered is dependent on length of time immobilized and the age of the individual.
Unlike reciprocating gait orthoses and passive standing devices, the ReWalk exoskeleton provides SCI paraplegics with the means to generate mechanical forces in their lower limbs that closely approximate the force patterns seen with normal ambulation. In one ReWalk clinical trial (9), an in-shoe pressure sensor was used to study the vertical ground reaction forces (vGRF) generated during ambulation for SCI participants and able-bodied volunteers. The effects of assistance during ReWalk ambulation were also examined. The magnitude of the mean vGRFs generated at heel strike, mid-stance and toe-off were not significantly different for the able-bodied controls and the SCI participants using the ReWalk with no assistance (Figure 4) (17, 18). The mean vGRF at heel strike was significantly lower for minimally assisted SCI participants as compared to the able-bodied controls. At mid-stance and toe-off, the mean vGRFs for the minimally assisted ReWalk group were significantly lower than the no assistance ReWalk group.
The mean vGRF profiles reported for each group follow the same trends, with similar force profiles seen for the unassisted ReWalk group and the able-bodied controls (Figure 5). While assistance decreased the vGRF, significant cyclic loading still occurred during walking for these participants. Generating compressive forces during weight bearing activities such as standing and ambulation using a variety of frames and orthoses have been reported to reverse calcium metabolism imbalances and improve BMD (19,20). Better restoration of the cyclic loads achieved by normal walking with the ReWalk exoskeleton may be more effective in mitigating the bone loss associated with long-term disuse in existing SCI individuals. Early intervention with ReWalk training and regular use of the device may help maintain lower limb bone mass for recently injured individuals and prevent the long term cortical bone loss that leads to fragility fractures.

Figure 4: Vertical round reaction force, expressed as per cent body weight, varied with stance phase and group (error bars represent 95% confidence intervals) (18). The body weight of the SCI groups was adjusted to remove the contribution of the device backpack and remote control watch. (*SCI min-assist vs. AB control: P=0.0034, SCI min-assist vs SCI no assist: P=0.0095 and 0.0457, respectively)
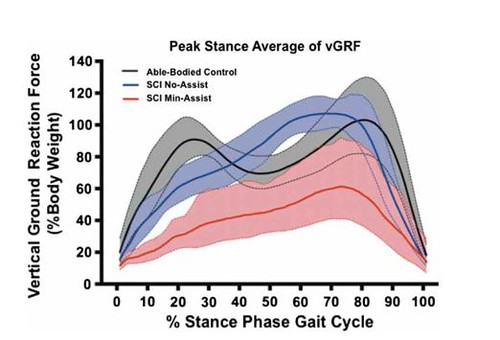
Figure 5: Vertical ground reaction force pattern during the gait cycle was similar for SCI with no assistance and able-bodied controls (18). Forces were lower for the minimally assisted group, although a cyclic variation in the force magnitude still occurred. (Error bands represent 95% confidence intervals.)
Seated Balance Improvements Resulting from ReWalk Use
Good seated balance skills are important for individuals affected by SCI, since the majority of their waking day is usually spent in a seated position. Developing and maintaining these skills enables the individual to perform an increased number of daily tasks independently. The influence of ReWalk use on seated balance was studied in initial participants in a ReWalk clinical trial (9, 21). These participants were tested prior to ReWalk training and again after an average of 28±16 training sessions were completed. For comparison, seven able-bodied volunteers were also tested. The Berg Balance Scale was used to assess static balance, while the modified function reach test, endpoint excursion (EPE), maximal excursion (MXE) and directional control (DCL) were used to assess dynamic balance.
Assessment prior to ReWalk use indicates that all of the dynamic balance parameters were significantly lower for the SCI participants as compared to the able-bodied controls (Figure 6). After ReWalk training, all dynamic balance parameters improved, with significant changes seen in the MXE and DCL dynamic balance measures (Figure 7). The greatest improvements were measured in forward and backward leaning balance (Figures 8 and 9), which may be associated with increased core muscle strength following ReWalk use. Improvements in muscle strength and control gained by upright mobility may also contribute to the reduced pain levels reported for participants in these trials.
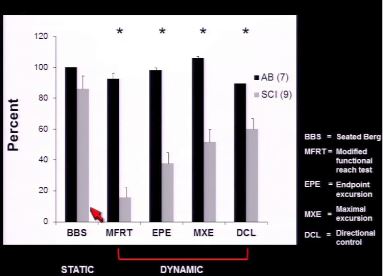
Figure 6: Assessment of static and dynamic seated balance prior to ReWalk training showed that dynamic balance parameters for the SCI participants were significantly reduced as compared to the able-bodied controls (21).

Figure 7: Dynamic seated balance parameters increased for SCI participants following ReWalk training. Statistically significant increases were measured in MXE and DCL (21).
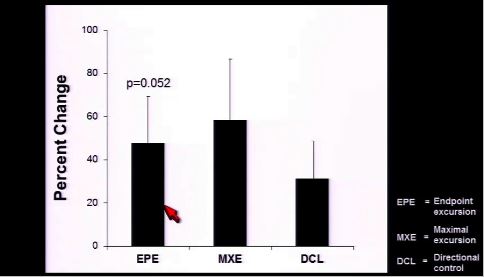
Figure 8: Front-leaning balance showed the greatest improvement following ReWalk training (21).
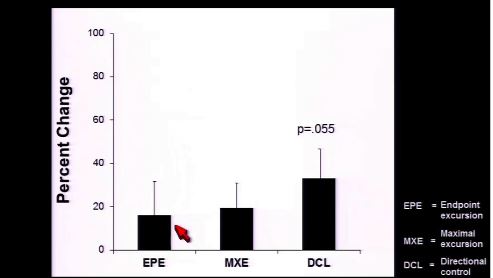
Figure 9: Back-leaning balance showed considerable improvement following ReWalk training (21). This improvement may be related to core muscle strength gained during training.
Quality of Life Benefits of ReWalk Use: Sleep
SCI can have significant secondary effects on quality of life. Many SCI individuals report difficulties sleeping at night, leading to excessive daytime fatigue and sleepiness. The effects of ReWalk use on fatigue level and sleep routine were assessed for clinical trial participants using three distinct measurement tools. The Epworth Sleepiness Scale (22) determines the level of daytime sleepiness. The Fatigue Severity Scale (23) measures the impact of fatigue on daily life. The PROMIS sleep disturbance measure (24) is a patient-reported assessment of nighttime sleep quality, sleep depth and restoration associated
with sleep. Participants were evaluated before their ReWalk user training sessions began and again after completing the training.
Sleep disturbances at night were significantly reduced following regular ReWalk use (Figure 10) (25). Using the ReWalk additionally resulted in a reduction in both the daytime sleepiness and fatigue measures, although these changes were not statistically significant at this point in the study (Figure 11).
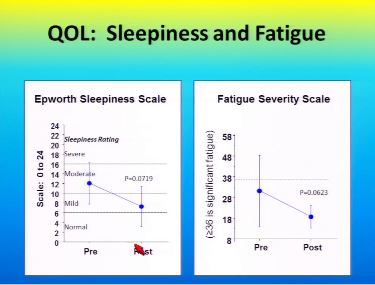
Figure 10: Sleepiness and fatigue were reduced following ReWalk training, although these reductions were not statistically significant at this point in the study (25).
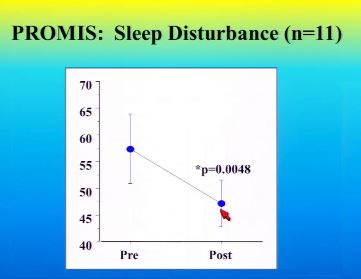
Figure 11: Nighttime sleep disturbances were significantly decreased following ReWalk training (25).
Quality of Life Benefits of ReWalk Use: Mental Outlook
Depression can have debilitating effects on SCI individuals, negatively impacting appetite, sleep, physical health and personal care. The mental health component of the SF-36 questionnaire was used to assess the effects of ReWalk use on the overall mental outlook of participants in an ongoing ReWalk clinical trial (9, 25, 26). The summary scores include perceived changes in vitality, social functioning, and emotional well-being. Prior to using the ReWalk, the summary score for the study participants was reported to be similar to previous evaluations of two groups of SCI individuals who were injured at least six months and less than four years. (Figure 12). The participant summary score increased following 40 ReWalk user training sessions as compared to the baseline and both reference groups, although only the latter difference is statistically significant at this point in the study.
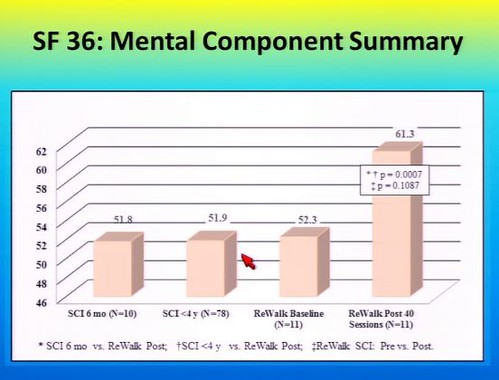
Figure 12: Comparison of the SF-36 mental component summary scores for study participants before ReWalk user training with other SCI individuals shows similar scores (25). After ReWalk user training, the mental component scores were significantly improved relative to individuals who did not participate in the study and also greater than the study participant baseline. However, the latter difference is not statistically significant at this point in the study.
Quality of Life Benefits of ReWalk Use: Pain
Pain following SCI can occur in regions of the body where sensation remains intact or where sensation is limited or absent. The etiology of this chronic pain is usually unknown, although it is most likely related to neural damage or musculoskeletal problems resulting from SCI. Chronic pain of this nature can interfere with daily activities and make personal interactions difficult. The effect of ReWalk use on pain levels was assessed before and after user training using the Spinal Cord Injury Quality of Life Measurement System (SCI-QOL) and the SF-36 questionnaire (9, 25-27). SCI-QOL pain behavior measures self-reported external manifestations of pain. These are verbal or non-verbal, involuntary or deliberate behaviors that typically indicate to others that an individual is experiencing pain. SCI-QOL pain interference measures the self-reported consequences of pain, specifically with regard to the extent to which pain hinders social, cognitive, emotional, physical, and recreational activities.
Mean pain behavior and pain interference scores were reported to decrease following ReWalk user training, although these reductions are not statistically significant at this point in the study (Figure 13). The SF-36 mean pain scores significantly increased after ReWalk user training for the same participant group, indicating a reduction in pain magnitude and interference (Figure 14). These improvements in pain levels may be related to strengthening of core muscles and better body conditioning following regular ReWalk use.
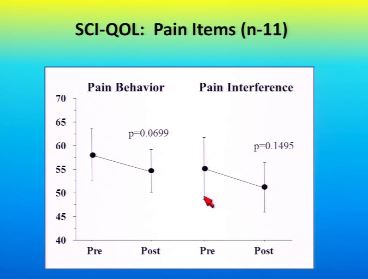
Figure 13: SCI-QOL pain measures decreased following ReWalk use, indicating reductions in the physical manifestations of pain and the impact of pain on physical and social activities of daily living (25).
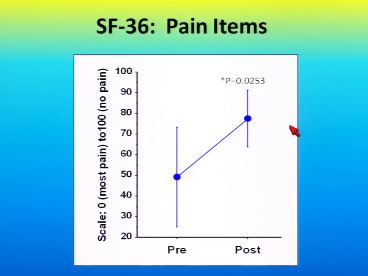
Figure 14: SF-36 mean pain score increased after ReWalk training, indicating a reduction in pain magnitude and effect (25).
Physiological Benefits of ReWalk Use: Physical Conditioning
Paraplegia resulting from spinal cord injury and the concomitant change to a sedentary way of life causes changes in body composition and muscle tone. Upright mobility using the ReWalk exoskeleton provides an opportunity for paraplegic individuals to regain conditioning through physical exertion. The heart rate for ReWalk users has been reported at specific points during user training sessions. Walking with the ReWalk increased the mean heart rate to approximately 85-119 beats per minute, which generally correlates to a moderate exercise level for able-bodied individuals (Figure 15) (32). An elevated heart rate was achieved throughout the training program, as participants were encouraged to progressively expand their mobility skills (Table 1). Participant rating of perceived exertion (RPE) decreased as walking distance and duration increased, indicating an increase in efficiency with increasing skill in using the device.
A comparison of energy consumption based on oxygen consumption was recently reported for the ReWalk exoskeleton and existing reciprocating gait orthoses (RGO) (17). Previous work demonstrated that RGOs create excessive energy demands, causing rapid fatigue. The energy expenditure for the powered ReWalk device is as much as 39% lower than values for RGOs reported in the literature (Table 2). Participants in the ReWalk trials were described as tolerating the device well for several hours per day.
Direct evidence for the physical benefit of walking with the ReWalk exoskeleton is seen in comparisons of body composition before and after the supervised user training sessions. ReWalk use was reported to significantly reduce fat mass and total body mass (Figure 16) over an average of 36 training sessions (approximately 12 weeks). Lean body mass increased concurrently, although this change was not statistically significant at this point in the study.
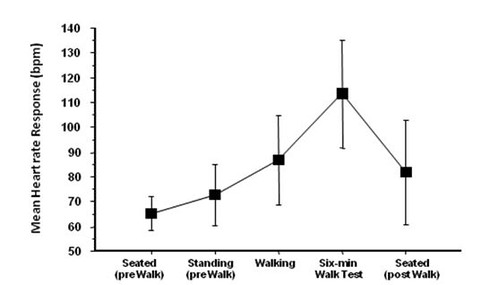
Figure 15: Mean heart rate during various ReWalk user training activities. Heart rate elevation during walking corresponds to a moderate exercise level for able-bodied individuals (26).
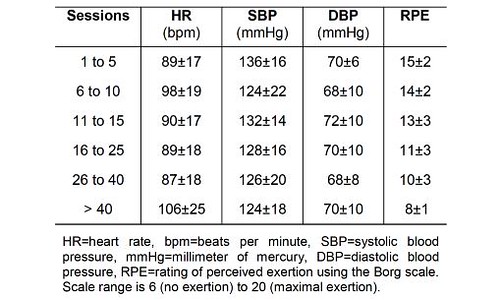
Table 1: Immediate Post-Walking Average Heart Rate, Blood Pressure and Rating of Perceived Exertion during ReWalk User Training Sessions (26).
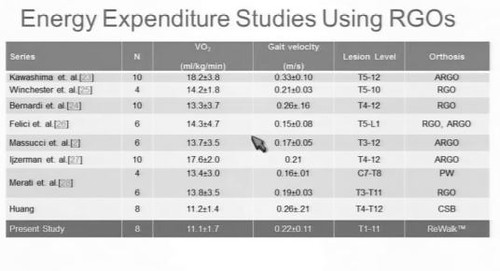
Table 2: Comparison of Energy Expenditure for RGOs and ReWalk (17).
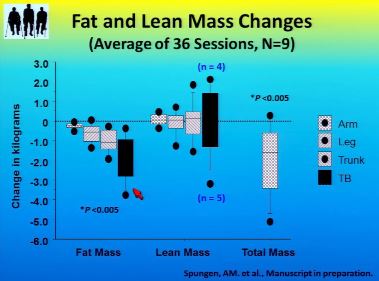
Figure 16: Overall and localized decreases in fat mass and total mass, and increases in lean body mass were seen after ReWalk user training (25).
Physiological Benefits of ReWalk Use: Pressure Ulcers
Chronic pressure ulcers are a significant problem for most individuals with SCI, since nerves that normally signal skin pressure are often damaged and concomitant paralysis limits voluntary weight adjustments to relieve the pressure. Constant pressure to focal areas of the skin restricts blood flow to the skin and subcutaneous tissues, leading to skin degradation and infection. It is generally accepted that virtually any method of repositioning and/or padding to provide relief from localized pressures should decrease the likelihood of developing a pressure ulcer (29-31). Repositioning options for individuals with SCI are limited however, since they spend the majority of their time sitting in a wheelchair or in bed. Upright mobility using the ReWalk exoskeleton provides an effective way to fully relieve skin pressure, particularly along the back and buttocks, and may help reduce the incidence and severity of pressure ulcers. Although the effect of ReWalk use on pressure ulcers has not yet been studied in a clinical trial, a study using a self-reported survey for SCI individuals who stood upright at least 30 minutes more than once per day reported a 33% reduction in pressure ulcers (8). As compared to standing, exoskeleton-assisted walking may be more effective at improving blood circulation and helping to maintain skin integrity.
Physiological Benefits of ReWalk Use: Bowel Function
Following spinal cord injury, the nerves controlling bowel function may be damaged such that bowel movements occur unplanned and reflexively, or the bowel may be flaccid and without muscular control. In either situation, a bowel management program is required for individuals with SCI to prevent accidental evacuations, as well as constipation, diarrhea and impaction. The effects of ReWalk use on bowel function were assessed using the SCI-QOL measure before and after completing user training. The results were recently reported for the first 11 participants in a ReWalk clinical trial (9, 25).
Bowel management difficulties decreased significantly (Figure 17) after ReWalk user training. Nine participants additionally reported the details of their bowel routine pre and post ReWalk training (Figure 18). Most participants experienced an increase in the number of bowel movements per day, a reduction in the time spent per day on bowel movements and a reduction in the number of bowel accidents per month. Eight of nine participants were able to reduce their use of laxatives, stool softeners, enemas and/or digital stimulation. ReWalk exoskeleton-assisted mobility was beneficial in improving bowel function for most participants despite variations in level of injury, length of injury (LOI), age, and sex.
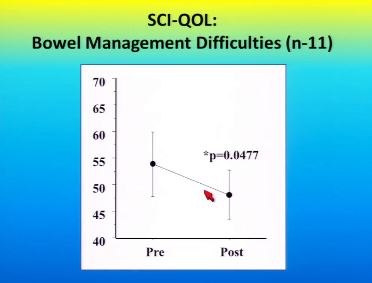
Figure 17: SCI-QOL assessment of bowel management difficulties before and after ReWalk training sessions (25). A significant improvement in bowel function occurred following ReWalk use.
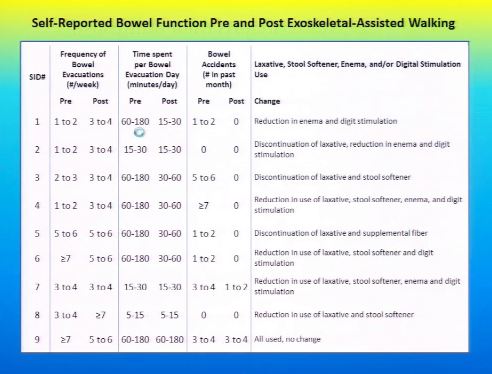
Figure 18: Reported changes in the bowel routines for participants in the ReWalk user training sessions (25). Most patients experienced improved bowel function following ReWalk use.
Physiological Benefits of ReWalk Use: Bladder Function
Urinary tract infection (UTI) is one of the most frequent causes of rehospitalization for individuals with SCI (33). Spinal cord injury alters the dynamics of bladder voiding, leading to conditions that increase the risk of UTI including bladder distention, high-pressure voiding, the presence of stones and retention of large post-void residuals (34). Both indwelling and intermittent catheterization significantly increase the risk of developing an infection. Persistent bacteriuria occurs within 30 days in 78-95% of SCI individuals with an indwelling catheter in place and 66% of SCI individuals maintained with intermittent catheterization develop bacteriuria (34, 35).
Increased physical activity is one approach that can be effective for decreasing the incidence of UTIs in individuals with SCI. A significant association between performing weekly exercises, the number of activities of daily living requiring assistance and the number of UTIs was demonstrated in one survey study (33). In a second randomized controlled clinical trial, the effects of more frequent and vigorous physical activity were examined (36). Participants received 16 weeks of aerobic training, one hour per session and up to three sessions per week. Training consisted of seated exercises such as upper limb work with a cycloergometer, wheelchair distance training and upper body muscle strengthening. At the start of the study, chronic asymptomatic bacteriuria was present in 61.9% of the control group and in 52.3% of the exercise group. At the end of the study, a statistically significant difference in the incidence of CAB was reported, with CAB present in 71.4% of controls and only 14.2% of the exercise group.
The effect of ReWalk use on bladder function was assessed as part of a clinical trial before and after ReWalk user training (9, 25). The SCI QOL measurement tool shows that bladder complications and management difficulties are significantly decreased following ReWalk training (Figure 19). Upright ambulation with the ReWalk exoskeleton may assist with more complete bladder voiding, helping to decrease the risk of UTI by reducing the amount of residual urine present in the bladder. Improved bladder function and a lower incidence of UTIs may also result from the improvements in seated balance that allow more independence with activities of daily living and the aerobic exercise provided by ReWalk use.
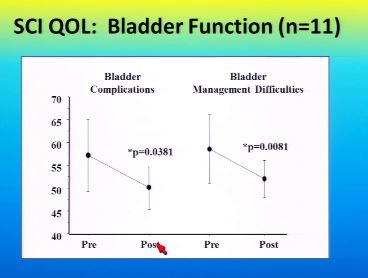
Figure 19: SCI-QOL assessment of bladder function before and after ReWalk user training sessions (25). There was a significant improvement in both bladder complications and bladder management difficulties following ReWalk use.
Medical Benefits of ReWalk Use
The benefits associated with regular use of the ReWalk exoskeleton to allow paraplegics with SCI to achieve upright mobility are summarized in Table 3.
Table 3: Medical Benefits of ReWalk Use.
|
ReWalk Benefit |
Summary of Data |
|
Maintenance of bone mass |
Walking with the ReWalk exoskeleton generates cyclic compressive loads similar in magnitude and pattern to the loads experienced by able-bodied individuals. These compressive loads may help maintain bone mineral density, reduce trabecular and cortical bone loss in the lower limbs, and decrease the incidence of fragility fractures in paraplegic individuals affected by SCI. |
|
Improved seated balance |
ReWalk use results in improved dynamic seated balance, particularly in forward and backward leaning positions. Increased core muscle strength and control may be gained, allowing greater functional independence with activities of daily living. |
|
Better sleep and reduced fatigue |
Nighttime sleep disturbances were significantly reduced following ReWalk use. Walking regularly several times per week with the ReWalk also reduced daytime sleepiness and fatigue. |
|
Improved Mental Health |
The mental outlook for participants in ReWalk clinical trials was significantly improved relative to SCI individuals who did not receive exoskeleton-assisted mobility training. |
|
Reduced pain |
External physical manifestations of pain and the impact of pain on daily personal and social activities were reduced after ReWalk user training. Pain may be alleviated by improvements in core muscle strength and body conditioning. |
|
Improved body conditioning |
Walking with the ReWalk exoskeleton increased the user’s heart rate to a level corresponding with moderate exercise for able-bodied individuals. The aerobic exercise provided by regular ReWalk use several times per week significantly reduced fat mass and total body mass. Lean body mass increased concurrently. |
|
Pressure Ulcers |
Upright mobility using the ReWalk exoskeleton provides physical exercise involving the entire body and allows full relief of back, buttock and leg skin pressure. Regular use of the ReWalk may help promote skin blood circulation and reduce the incidence and severity of pressure ulcers. |
|
Improved bowel function |
ReWalk exoskeleton-assisted mobility was beneficial in improving bowel function for most users regardless of variations in level of injury, length of injury, age, and sex. Time spent on bowel management was reduced, along with the need for medical or manual bowel stimulation. |
|
Improved bladder function and reduced risk of UTI |
Bladder complications and management difficulties were significantly decreased following ReWalk use. Upright mobility may assist with more complete bladder voiding, helping to decrease the risk of UTI. The aerobic exercise provided by regular ReWalk use, leading to improved body conditioning and better seated balance, may also lower the incidence of UTIs. |
References
- https://www.nscisc.uab.edu/PublicDocuments/fact_figures_docs/Facts%202014.pdf
- S. Fritz, M. Lusardi: Walking Speed: The Sixth Vital Sign. J. Ger. Phys. Ther. 32:2-5, 2009
- H.J. Van Hedel: Gait Speed in Relation to Categories of Functional Ambulation after Spinal Cord Injury. Neurorehabil. Neural Repair 23(4):343-50, 2009
- B. Morganti, G. Scivoletto, P. Ditunno, J.F. Ditunno, M. Molinari: Walking Index for Spinal Cord Injury (WISCI): Criterion Validation. Spinal Cord 43(1):27-33, 2005
- J. Opara, K. Mehlich, A. Bielecki: Walking Index for Spinal Cord Injury. Ortop. Traumatol. Rehabil. 9(2):122-7, 2007
- http://www.heart.org/HEARTORG/GettingHealthy/PhysicalActivity/Walking/Why-Walking_UCM_461770_Article.jsp
- http://www.heart.org/HEARTORG/GettingHealthy/PhysicalActivity/Walking/Walking-101_UCM_461766_Article.jsp
- J.S. Walter, P.G. Sola, J. Sacks, Y. Lucero, E. Langbein, F. Weaver: Indications for a Home Standing Program for Individuals with Spinal Cord Injury. J. Spinal Cord Med. 22(3): 152-158, 1999
- A.M. Spungen: The ReWalk Exoskeleton Walking System for Persons with Paraplegia (VA_ReWalk). In: ClinicalTrials.gov. Bethesda MD: National Library of Medicine (US). https://www.clinicaltrials.gov/ct2/show/NCT01454570?term=Rewalk&rank=4
- A.M. Spungen: Home/Work Community Skills in the ReWalk Exoskeleton in Persons with SCI (VA_ReWalk2). In: ClinicalTrials.gov. Bethesda MD: National Library of Medicine (US). https://www.clinicaltrials.gov/ct2/show/NCT02118194?term=Rewalk&rank=3
- D.R. Carter: Mechanical loading histories and cortical bone remodeling. Calcif. Tiss. Intl. 36:S19-24, 1984
- L.E. Lanyon: Functional strain as a determinant for bone remodeling. Calcif. Tiss. Intl. 36: S56-61, 1984
- M. Dauty, B. Perrouin Verbe, Y. Maugars, C. Dubois, And J. F. Mathe: Supralesional and sublesional bone mineral density in spinal cord-injured patients. Bone 27(2):305-9, 2000
- Y. Zehnder, M. Lu, D. Michel, H. Knecht, R. Perrelet, I. Neto, M. Kraenzlin, G. Za, K. Lippuner: Long-term changes in bone metabolism, bone mineral density, quantitative ultrasound parameters, and fracture incidence after spinal cord injury: a cross-sectional observational study in 100 paraplegic men. Osteoporosis Intl. 15:180-9, 2004
- A.D. LeBlanc, E.R. Spector, H.J. Evans, J.D. Sibonga: Skeletal responses to space flight and bed rest analog: A review. J. MusculoSkel. Neuro. Intact. 7(1): 33-47, 2007
- V.S. Schneider, J. McDonald: Skeletal calcium homeostasis and countermeasures to prevent disuse osteoporosis. Calcif. Tiss. Intl. 36:S151-4, 1984
- P. Asselin: Exoskeleton Assisted Walking: Training methods and mobility skills achieved. Presented at Amer. Acad. Phys. Med. Rehabil. 2014 Annual Assembly, 213-AAPMR-14
- D.B. Fineberg, P. Asselin, N.Y. Harel, I. Agranova-Breyter, S.D. Kornfeld, W.A. Bauman, A.M. Spungen: Vertical ground reaction force-based analysis of powered exoskeleton-assisted walking in persons with motor-complete paraplegia. J. Spinal Cord Med. 36(4):313-21, 2013
- S. Goemaere, M. Van Laere, P. De Neve, J.M. Kaufman: Bone mineral status in paraplegic patients who do or do not perform standing. Osteoporosis Intl. 4:138-43, 1994
- P.E. Kaplan, B. Gandhavadi, L. Richards, J. Goldschmidt: Calcium balance in paraplegic patients: influence of injury duration and ambulation. Arch. Phys. Med. Rehabil. 59(10): 447-50, 1978.
- N.Y. Harel, P.K. Asselin, S. Knezevic, S.D. Kornfeld, A.M. Spungen: Exoskeleton walking improves seated balance in chronic SCI. Presented at Amer. Acad. Phys. Med. Rehabil. 2014 Annual Assembly, 213-AAPMR-14
- M.W. Johns: A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 14(6):540-5, 1991.
- G.B. Neuberger: Measures of fatigue. Arthr. Rheum. 49(5S):S175-S183, 2003
- http://www.nihpromis.org
- A.M. Spungen: Exoskeleton-assisted walking for persons with spinal cord injury. Presented at Amer. Acad. Phys. Med. Rehabil. 2014 Annual Assembly, 213-AAPMR-14
- A.M. Spungen, P.K. Asselin, D.B. Fineberg, S.D. Kornfeld, N.Y. Harel: Exoskeleton-assisted walking for persons with motor-complete paraplegia. NATO Science and Technology Organization, STO-MP-HFM-228 pp.6-1 – 6-14, 2013
- M.P.J.M. Dijkers: Quality of life of individuals with spinal cord injury: a review of conceptualization, measurement and research findings. J. Rehabil. Res. Dev. 42(3):87-110, 2005
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 30(6):473–83, 1992
- Henzel MK, Bogie KM, Guihan M, Ho CH. Pressure ulcer management and research priorities for patients with spinal cord injury: Consensus opinion from SCI QUERI Expert Panel on Pressure Ulcer Research Implementation. J Rehabil Res Dev. 2011; 48(3):xi-xxxii
- S.L. Groah, M. Schladen, C.G. Pineda, C.H. Hsieh: Prevention of pressure ulcers among people with spinal cord injury: a systematic review. PM&R, Published Online: December 18, 2014
- Pressure ulcer prevention: an evidence-based analysis. Ont. Health Technol. Assess. Ser. 9(2):1-104, 2009
- http://www.cdc.gov/physicalactivity/everyone/measuring/heartrate.html
- T. Kroll, M.T. Neri, P.S. Ho: Secondary conditions in spinal cord injury: results from a prospective study. Disabil. Rehab. 29(15):1229-37, 2007
- D.D. Cardenas, T.M. Hooton: Urinary tract infections in persons with spinal cord injury. Arch. Phys Med. Rehab. 76:272-80, 1995
- A. Esclarin De Ruz, E. Garcia Leoni, R. Herruzo Cabrera: Epidemiology and risk factors for urinary tract infection in patients with spinal cord injury. J. Urol. 164:1285-9, 2000
- E.L. Lavado, J.R. Cardoso, L.G.A. Silva, L.F. Dela Bela, A.N. Atallah: Effectiveness of aerobic physical training for treatment of chronic asymptomatic bacteriuria in subjects with spinal cord injury: a randomized controlled trial. Clin. Rehab. 27(2):142-9, 2012
Click Your Level of Injury